Healthcare Quality and Outcomes Lab Assesses Impact of Homelessness Comorbidity Payments

Since October 2023, the Centers for Medicare and Medicaid Services (CMS) has designated homelessness as a complication or comorbidity (CC) affecting inpatient medical care. This designation reflects evidence that people experiencing homelessness face substantially worse health outcomes and higher acute care use than comparable patients without homelessness.
CMS designates a diagnosis as a CC when it is expected to increase resource use in the inpatient setting, and reimbursement is adjusted upward when at least one CC is documented. The CC class is broad, encompassing conditions such as diabetes, pneumonia, and, since October 2023, homelessness. For most CCs, assignment relies on standard clinical ICD-10 diagnosis codes; for homelessness, the relevant codes are ICD-10 “Z codes,” which capture social determinants of health.
Proposed policy changes
CMS has proposed reversing this additional reimbursement for homelessness, beginning in October 2026. Homelessness is one of two groupings of Z codes that CMS currently designates as CCs; the other, housing insecurity, is also slated to revert to non-CC status.
The rationale CMS offers is that these Z codes “describe social circumstances and not medical conditions or illnesses.” The proposed rule quantifies the additional reimbursement attributable to CC status but does not assess the classification’s documentation effects.
Our research
A research letter published last week in JAMA Network Open by our group examines the effects of the 2023 homelessness classification. We document two effects of the policy on inpatient Z code use:
- A broad acceleration in the documentation of housing insecurity, food insecurity, financial insecurity, and transportation insecurity over the year after homelessness became a CC, despite no payment incentive attaching to those codes.
- An immediate level increase in homelessness documentation of 1.02 events per 1,000 hospitalizations — an 18.0% relative increase from the pre-CC baseline.
In our paper, led by Josh Calianos, Jose Figueroa, and the Healthcare Quality and Outcomes Lab team, we drew on 100% Medicare fee-for-service claims covering 13.9 million hospitalizations at 4,612 hospitals. We assessed differences between the 12 months before the policy took effect (October 2022–September 2023) and the 12 months that followed (October 2023–September 2024).
Figure 1: Unadjusted Monthly Documentation Rate of Z Codes for Homelessness, Housing Insecurity, and Other Health-Related Social Needs Per 1,000 Hospitalizations Among Traditional Medicare Beneficiaries, 2022–2024
Shaded area indicates the period during which homelessness was billable as a CC
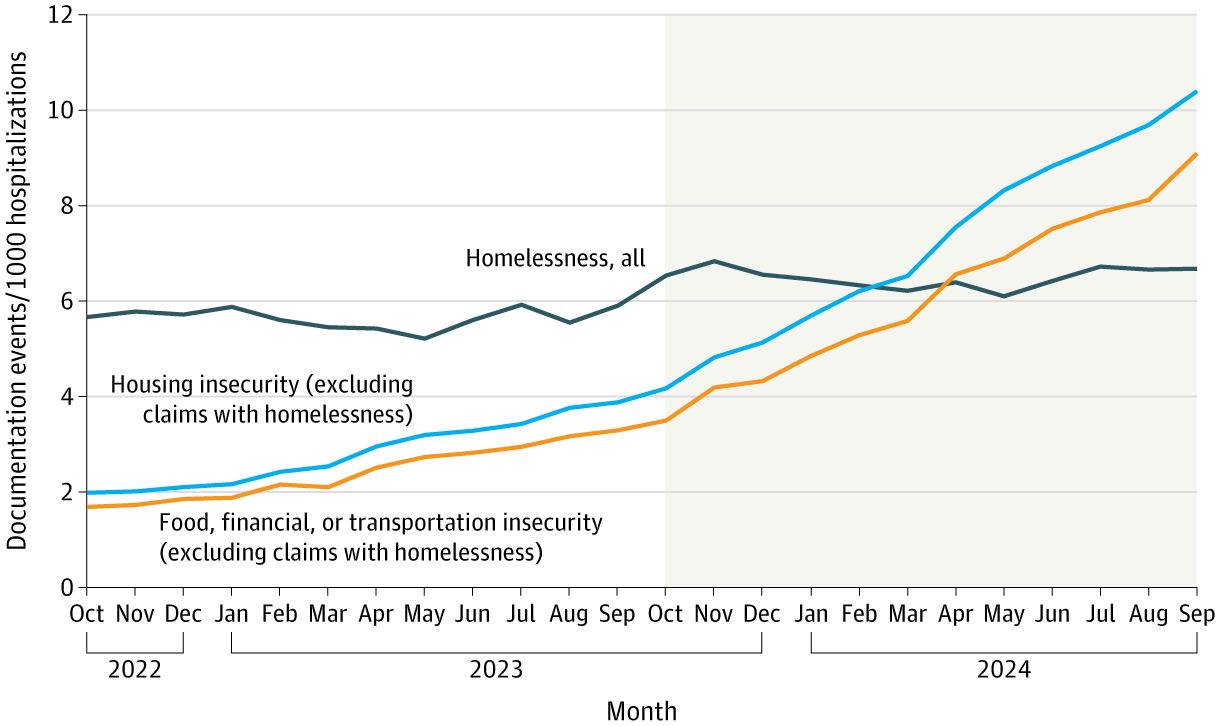
In the October 2023–September 2024 period, the largest documentation changes compared with October 2022–September 2023 were in Z codes that carried no direct payment incentive (Figure 1).
Documentation of housing insecurity Z codes (which were themselves elevated to CC status in October 2024) rose from 1.69 to 9.10 events per 1,000 hospitalizations, with a significant acceleration in the monthly slope after October 2023.
Documentation of food, financial, or transportation insecurity Z codes followed a parallel course, rising from 1.99 to 10.40 events per 1,000 hospitalizations. The inflection point for both trajectories aligns with the October 2023 policy boundary.
Documentation of homelessness itself rose more modestly, from 5.66 to 6.68 events per 1,000 hospitalizations, although this was an 18.0% relative increase. The underlying slope of homelessness documentation did not change significantly between the pre- and post-policy periods, so the level shift is consistent with a discrete effect of the policy rather than a continuation of prior trends.
These patterns describe an effect of the CC designation that extends beyond the reimbursement question CMS’s rule directly addresses.
These accelerations cannot be cleanly attributed to the homelessness reclassification alone. A contemporaneous CMS mandate requiring hospitals to screen for health-related social needs took effect in 2024, and other recent work documents independent associations between the screening mandate and inpatient Z code activity. However, the immediate level shift we observed in homelessness documentation at the October 2023 policy boundary provides evidence of an effect attributable to the reclassification itself.
Assessing the full impact of the CC classification
CMS’s proposal rests on the assertion that social determinants of health should not be reimbursed like chronic medical conditions. However, the proposal also sits in tension with CMS’s own broader policy direction. Since 2024, the agency has required hospitals to screen inpatients for health-related social needs under its Inpatient Quality Reporting program. Reversing the CC designation would withdraw a payment signal that appears to be reinforcing the documentation behavior the screening requirement itself was designed to elicit, even as the screening requirement remains in place.
Homelessness appears to increase costs similarly to other CCs. CMS shows in a resource-use analysis that hospital stays where homelessness is the only CC/MCC (major complication or comorbidity) consume 1.76 times the resources of admissions with no CCs or MCCs. This finding may actually support retaining the designation because it compensates hospitals for a resource burden CMS has acknowledged.
The marginal payment effect may be larger than the CMS analysis implies. The homelessness documentation increase we observed was concentrated among non-dual-eligible beneficiaries, patients who were less likely to present with another CC or MCC. Because incremental reimbursement attaches only to the first documented CC or MCC, the homelessness designation carries marginal billing value for this subset.
The benefits of documenting homelessness and adjacent social determinants of health extend beyond hospital reimbursement. Our paper documents an immediate, statistically significant increase in homelessness documentation, alongside a broader acceleration in the documentation of other social determinants of health. The broader acceleration likely reflects multiple contributing factors, including CMS’s 2024 screening mandate. But even setting it aside, the direct level shift in homelessness documentation, combined with the resource-use evidence CMS itself offers, provides reason to preserve the designation.


