What Rural Kenya Taught Me About Designing Interventions That Go Beyond the Pilot
Sonali Verma is a Rose Service Learning Fellow and a Master of Public Health candidate in the Department of Global Health and Population.
As a health systems researcher hoping to amplify the voices of patients and healthcare workers in Sub-Saharan Africa, I received a piece of advice that stuck with me: “Let Kenyans tell Kenyan stories.” The words came from the founder of The Leo Project, Jess Danforth, a cancer survivor who completed the Harvard MPH Generalist program while living in Kenya. As a fellow cancer survivor, I’m deeply grateful for the opportunity to co-design cancer care pathways grounded in community needs, learning alongside Kenyan cancer champions and advocates.

In Kenya, 68% of the population lives in rural areas. The Leo Project (TLP) serves 22 rural villages across Laikipia County spanning more than ten tribes – including Kikuyu, Maasai, Samburu, and Meru – which means cultural context and language shift from one community to the next. In my eight years of global health research spanning six countries, I have yet to encounter a model of primary care as authentically community-centered as The Leo Project. What struck me most wasn’t only the ambition of building a cancer center for a county where more than 500,000 people lack access to cancer care. It was the model behind it: a model of people-centered care where community voice drives the design from the ground up.

When Jess is asked why a primary care organization invests in water towers or digital literacy, especially given the challenge of “scaling” health services, her answer is simple: health doesn’t exist in silos. TLP’s work treats the community as the unit of design, not the clinic. And that shift – from facility-centered to people-centered – changes what becomes possible. This approach has positively impacted health-seeking behavior, driving more than 21,000 patient visits. People-centered care can be built to scale – even amidst the resource constraints across rural Kenya.
Reframing Last Mile “Resource Constraints”
Experiencing this model forced me to rethink what global health practitioners mean when we label a setting “resource-constrained.” What is truly scarce – and what have we chosen not to value?
From far away, it’s easy to default to a narrative of injustice and breakdown: victims of broken systems, grim statistics, and scarcity. In public health classrooms, we highlight numbers that capture inequity, such as “80% of people in Kenya are diagnosed with cancer at a Stage 3 and 4.” We lean on frameworks, case studies, and cross-country comparisons to explain why. Those tools matter. But when we center only on system failure, we can unintentionally flatten communities instead of recognizing agency. Often, global health narratives overlook the fact that capability already exists within communities. People are living these challenges everyday and, against many odds, finding practical, inventive solutions in their own backyard. Our role is to help surface, connect, and strengthen what is already there. Community health leaders, survivor advocates, and grassroots organizations are the engines of real change in Laikipia County, improving health outcomes in ways that rarely make it into formal reports.
One of the clearest examples is Brian, a cancer survivor who has become a local catalyst who runs prosthetic-knitting support sessions for more than 60 survivors at a donation-supported palliative care center.

He is training cancer survivors across villages to lead outreach as Certified Cancer Awareness Volunteers (CAVs). We worked with community members to co-design patient navigation models grounded in real barriers and lived experience. Our defining principle: “Diagnosis without navigation is not care.” Again and again, oncology nurses and community health promoters voiced that survivors can dispel myths and reframe cancer as treatable – not a death sentence – more effectively than health workers alone. When a trusted peer speaks – say, a Maasai cervical cancer survivor talking with a Maasai woman – here’s instant credibility: “someone like me,” who understands the local realities behind care-seeking, from cancer myths and female genital mutilation (FGM) to stigma and the everyday burdens pastoral families carry. That trusted relationship can move behavior more powerfully than information alone.
Reframing the Goal for Scale from the Start:
At Harvard Chan’s Global Health & Population program, we are trained to design interventions that scale – national rollouts with Ministries of Health, regional resource allocation under tight budgets, and the hard work of moving beyond pilots.
For the past eight years, I’ve applied that lens in private-sector health technology, designing and deploying AI imaging and diagnostic tools in last-mile communities. Even when teams acknowledge that no single approach fits every context, every Health AI company I’ve worked with still wants an “implementation playbook”: a distilled set of cross-health system lessons on what consistently works, what fails, and what to adapt – built to support scale.
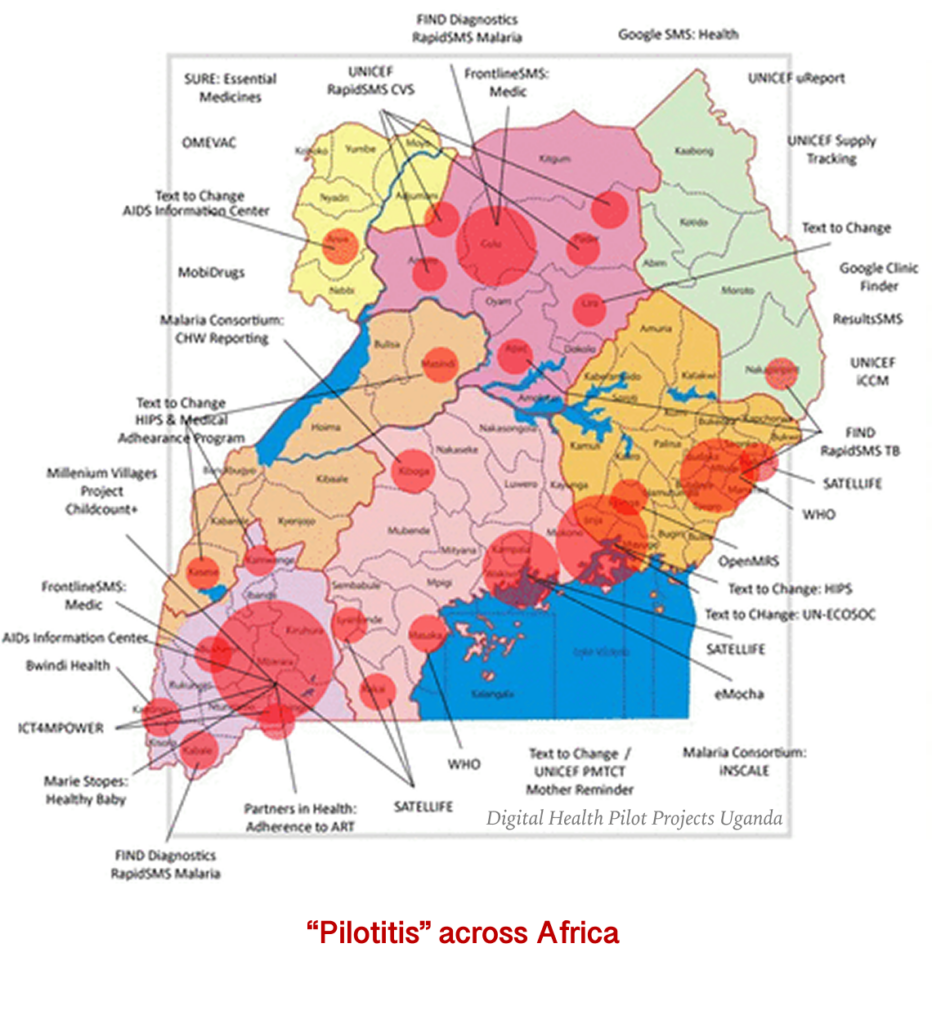
Laikipia reinforced an overlooked truth in the health tech sector: scale that improves health is impossible without deep local context and real ownership from community partners. When urgency to scale replaces local inquiry, we lose the context that drives adoption and impact. That gap fuels “pilotitis”: promising pilots that never sustain or scale.
“Implementation playbooks” shouldn’t simply import best practices – they should standardize how we learn locally, so communities can lead, design, adapt, and own what lasts. This is what makes interventions durable across generations, beyond the five-year pilot. Bottom line: technology matters, but people and systems are what determine outcomes.
I am deeply grateful for the Rose Service Learning Fellowship and The Leo Project that gave me the opportunity to meaningfully engage with a global community of changemakers who shifted my perspective. And thankful to Harvard Alumni, Jess, through whom I gained not only lessons to shape my future career, but a mentor for life.

