Ariadne Labs’ TeamBirth model empowers mothers, improves outcomes
In hundreds of labor and delivery units across the U.S. and beyond, patients and clinicians are benefiting from TeamBirth, Ariadne Labs’ caregiving model that promotes teamwork, communication, and dignity
Obstetric nurse and Harvard T.H. Chan School of Public Health research scientist Amber Weiseth compares Cesarean section rates to a dashboard warning light in a car. If you want to understand how a maternal health care system is performing, she says, check out how many patients are giving birth via C-section. An extremely high number signals a problem.
Clinician-researchers at Ariadne Labs—a joint center for health systems innovation at Brigham and Women’s Hospital and Harvard Chan School—have seen this warning light go on. In the U.S., the rate of C-sections—an often lifesaving procedure for mothers and infants—increased 500% between 1965 and 2010. Yet in that time, the country’s maternal mortality rate also increased sharply, more than doubling between 1987 and 2009 and disproportionately impacting women of color, particularly Black women.
So in 2013, Ariadne researchers began investigating what was driving these concerning–and sometimes tragic–outcomes, determined to find answers that could inform solutions.
In the last 13 years, Ariadne’s research has done just that. The team has exposed cracks in maternal health systems that have contributed to high C-section rates. And in 2016, after convening a group of community members, doulas, clinicians, and maternal health experts, they developed a solution to help fill those cracks: TeamBirth, a caregiving model that uses “huddles” to bring clinicians and patients together in shared communication throughout childbirth.
Hundreds of hospitals in the U.S., and more than a dozen internationally, have implemented TeamBirth. Across these labor and delivery units, C-section rates have begun to decline. What’s more, trust and autonomy is rising among patients—particularly those belonging to racial minorities—and among clinicians.
“Yes, we wanted to drive C-section rates down, because we don’t want to continue overusing major surgery,” said Weiseth, who joined Ariadne in 2018 and leads the design, implementation, and research of TeamBirth. “But more so we wanted to figure out the problems behind overuse of C-sections, and how to flush those problems out. Because we thought those same problems may be contributing to other bad and sometimes much more serious outcomes, like maternal death.”

The pressure tank model
While there’s no definitive rate at which C-sections do more harm than good, Ariadne’s research found a point at which the benefits of the procedure level off. Comparing countries’ maternal and neonatal health outcomes, they concluded that women and infants do not fare better in countries where the national C-section rate exceeds 19%. The U.S. C-section rate has hovered around one in three for the last decade, but with great variation across hospitals. Some hospitals deliver just 10% of infants via C-section; others, more than 40%.
These wide variations didn’t appear to be due to conventional explanations, the researchers found. It wasn’t the case that hospitals performing more C-sections had a higher number of complicated patients or patients who preferred the procedure. Nor was insurance a factor.
Instead, the researchers found, C-section rates were largely a product of how much pressure a labor and delivery ward faces. They deemed it the “pressure tank model”: high patient volumes, limited staff, and the volatility of labor and delivery create a complex, stressful, busy environment where communication is difficult and teamwork erodes. As a result, clinicians opt to perform C-sections, even when medically unnecessary, rather than letting patients continue to progress in labor. C-sections are faster, requiring fewer nursing hours at the bedside. And, once the procedure begins, clinicians no longer have to communicate back and forth as much to make decisions about a case.
“Research has demonstrated that the more dysfunctional a team is, and the more negative culture is within a labor and delivery unit, the more C-sections there are,” Weiseth said. “It makes sense, right? If people aren’t working well together, they’re going to use the release valve of a C-section more often.”
The team found other culprits driving too-high C-section rates, including financial pressures—obstetric care as a whole is poorly reimbursed and C-sections earn more money than vaginal deliveries—and inconveniently designed wards, with too many rooms placed too far away from each other, cutting off communication between clinicians.
But these issues weren’t as solvable. So without redesigning insurance schemes or hospital facilities, Ariadne researchers set their sights on teamwork: improving how labor and delivery staff could communicate and collaborate better.
TeamBirth isn’t a high-tech innovation. It’s about enabling better communication and decision-making between everyone in the labor and delivery ward, including patients. It’s really about culture change, introducing efficiency where there was inefficiency, thoroughness where there was rush, and connectedness where there was detachment, or even disagreement or conflict.
Amber Weiseth, director of TeamBirth
‘Back at the bedside’
How could labor and delivery units transform into environments where clinicians communicated efficiently? How could teams overcome the fast pace and pressure of the ward to regularly connect and collaborate—not only with each other, but also with their patients?
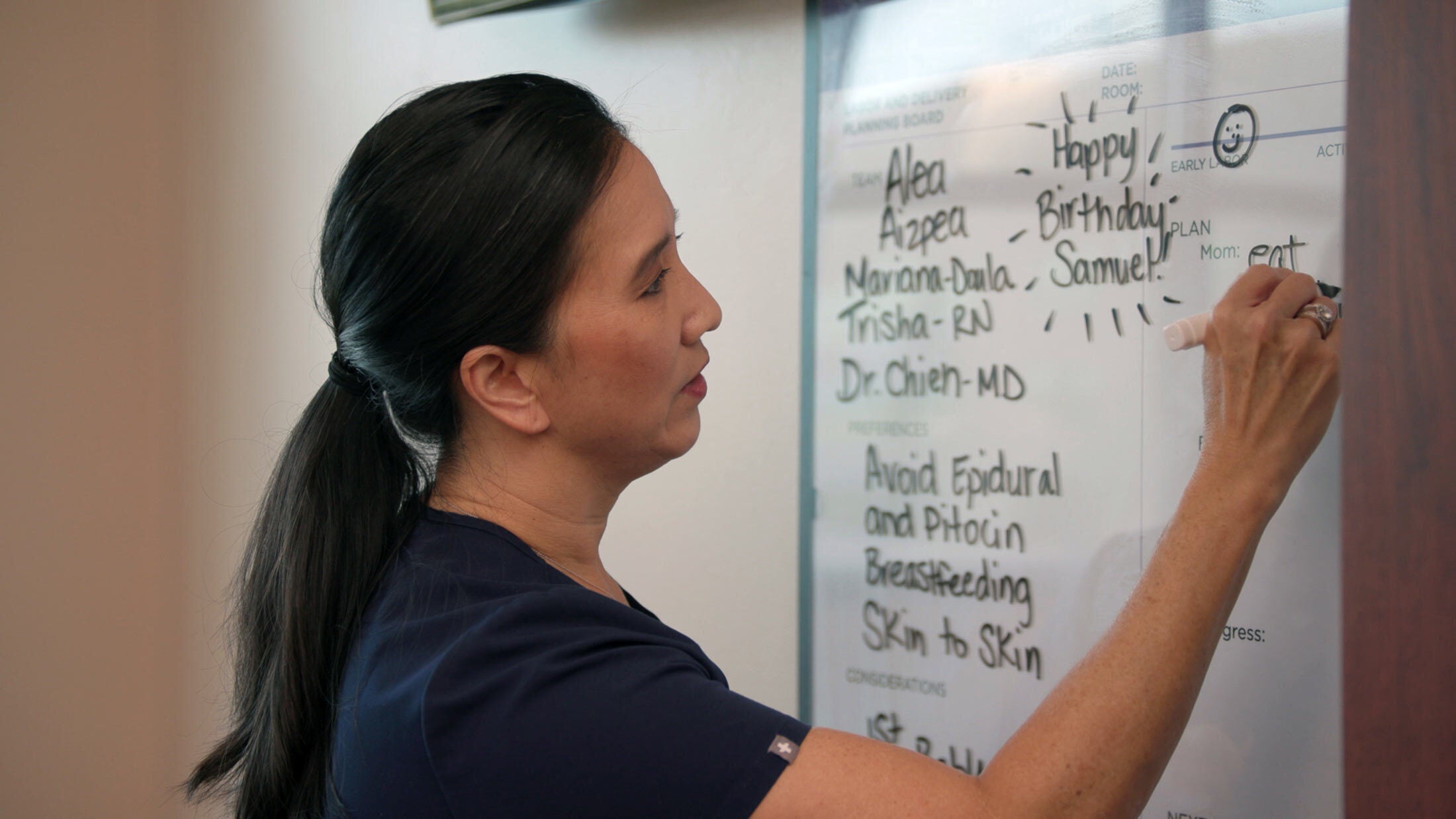
Those questions gave rise to TeamBirth. Under the model, from the time a laboring patient is admitted until she is discharged, she, her nurse, her physician or midwife, and her support people such as a partner or doula, “huddle” to make decisions at regularly established intervals. As a team, they discuss progress, share their experiences and expertise, decide on any changes to care plans, and schedule their next huddle. And they record it all on a whiteboard that everyone can refer back to.

“At its core, TeamBirth reflects an elegant human simplicity: It enables caring that maintains dignity,” said Asaf Bitton, executive director of Ariadne Labs and associate professor of health care policy at Harvard Chan School. “It makes intuitive sense not just to clinicians, but to anyone who has experienced health care, because it addresses a fundamental truth—when systems fall short, it’s often a failure of connection, communication, and care.”
“It isn’t a high-tech innovation,” Weiseth added. “It’s about enabling better communication and decision-making between everyone in the labor and delivery ward, including patients. It’s really about culture change, introducing efficiency where there was inefficiency, thoroughness where there was rush, and connectedness where there was detachment, or even disagreement or conflict.”
Weiseth and her team—a group of nurses, midwives, obstetricians, project managers, research specialists, and coordinators—are regularly approached by hospitals looking to implement TeamBirth, and they generally work with each for about a year to do so.
“Setting up white boards is easy. But it’s not really about that. We’re talking about change management,” she said. “It can take months to train a unit’s full staff, and many more to observe if and how behaviors are shifting. We help hospitals troubleshoot through that process and collect troves of data to monitor impact.”
To date, more than 300 hospitals in the U.S., and more than a dozen in Canada, Sweden, Nepal, Switzerland, and Brazil, are implementing TeamBirth. Five states—Washington, New Hampshire, Oklahoma, New Jersey, and Nebraska—are scaling the program statewide.
The results have been promising: High C-section rates are dropping at these hospitals. At one in Oklahoma, for example, 24% of low-risk patients now deliver via C-section, down from 33% pre-TeamBirth.
In addition, in Ariadne’s surveys on clinician and patient experiences with TeamBirth, clinicians have reported greater job satisfaction, work culture, and team harmony. They’ve noted that TeamBirth has helped emphasize the value of input from nurses, and fostered safer environments in which to voice a concern about a patient’s care. Nearly all of them—94%—agreed that TeamBirth improved care for laboring patients.
“For clinicians, if you improve teamwork, it makes their job easier and more enjoyable,” Weiseth said. “They get to be back at the bedside, truly connecting with patients and their colleagues. For so many of them, TeamBirth reminds them why they went into health care and also enables them to give the kind of care they want to give.”
Reducing racial disparities
TeamBirth is also facilitating the kind of care patients want to receive. In surveys, the vast majority of TeamBirth patients have reported high levels of autonomy and confidence in their care team, greater than the levels reported by non-TeamBirth patients. And while these improvements in care are benefiting every patient who delivers at a TeamBirth hospital, Ariadne researchers have found that the greatest changes are among patients belonging to racial minorities—those who bear the brunt of maternal mortality and mistreatment in hospitals.
Among Black patients who had a TeamBirth huddle, 89% said they felt a high level of autonomy—nearly 30 percentage points more than those who did not have a huddle. And many hospitals’ C-section rates are decreasing in accordance with the closing of massive racial disparities in maternal care. At a hospital in Cleveland, for example, C-section rates were 41% for Black patients and 27% for white patients before the implementation of TeamBirth. After, they were 22% and 23%, respectively.
“I truly believe clinicians come to work every day with the intent to make the best decisions and to care for patients unbiasedly. This is a model that helps them do that,” Weiseth said. “It helps correct implicit biases and standardizes the way they provide care and make decisions, so they’re able to be their best selves in every interaction with every patient.”
Weiseth recalled one TeamBirth case that illustrated the model’s benefits. A Black patient arrived at a rural hospital to be induced with two doulas at her side—an unusual occurrence, one that signaled fear and mistrust. “There was friction during the admission process, but that all went away once a nurse who’d just been trained on TeamBirth initiated the patient’s first huddle,” Weiseth said. “The nurse brought everyone together, and things slowed down to be able to really center the woman in her care. The woman went on to safely give birth and later wrote, ‘TeamBirth cleared some misunderstandings that I had at the beginning. What a healing experience.’”
“Here’s someone who entered the health system not feeling safe or like she could trust her clinicians, and someone who statistically is likelier to have a bad outcome,” Weiseth continued. “But because these clinicians met her and listened to her and made decisions with her, she not only had a good outcome, but felt healed in the process—and is much more likely to seek care again in the future. This is all exactly what we’re hoping to achieve, exactly how we’re hoping to fix issues within maternal health systems.”

Scaling up
As TeamBirth expands into more states and internationally, it’s also spreading to postpartum wards and neonatal intensive care units. Many patients who received TeamBirth care were disappointed to no longer have huddles in the moments and days after having their baby—and many hospitals have responded accordingly.
Weiseth said hospitals have also asked about spreading TeamBirth to other units in the hospital—different name, same model. Some have already begun doing so. Ariadne researchers are hoping to collect data on these efforts, to understand if, where, and how the TeamBirth model is effective outside of maternal health care.
“We need to be able to provide evidence for TeamBirth to be scaled broadly,” Weiseth said. “But the model of care is not a unique need in obstetrics. It’s really about how to make decisions in complex health care situations, how to center patients, and how to get people to talk to each other. Because once you get people to talk to each other, it brings to light the issues—cultural, hierarchical, procedural, policy—that are creating any and all poor health outcomes. Not just unnecessary C-sections. That’s where we started, but it’s not where we remain solely focused. We’re actually trying to change the whole health system.”


