Military Community Potentially Exposed to Hospitals at Higher Risk of Financial Distress

Written by Josh Calianos, Jessica Phelan, Jose Figueroa*, and Thomas Tsai*.
* Faculty at Harvard T.H. Chan School of Public Health; Principal Investigators of the Healthcare Quality and Outcomes Lab
Medicaid Cuts, Hospital Closures, and Care for Military Personnel, Veterans, and Families
Introduction
Military personnel, veterans, and their families rely heavily on civilian hospitals for healthcare, particularly in areas without military treatment facilities. TRICARE, the military health insurance program, provides healthcare for members of these groups at civilian hospitals when military treatment facilities (MTFs) are unavailable or lack specialized services.
As the Department of Defense has planned to shrink the footprint of MTFs, the number of TRICARE beneficiaries purchasing care at civilian hospitals is expected to grow. While the exact scope of this realignment is still unclear, the fiscal year (FY) 2026 National Defense Authorization Act acknowledged this process and set requirements for the Defense Health Agency to follow as it downsizes MTFs.
Access to Civilian Hospitals by Active-Duty Service Members and Families
Active-duty service members and their families often receive care from civilian hospitals even when they live on an installation with a hospital. More than 4,600 civilian acute care hospitals accepted TRICARE in 2023. Service members also utilize outpatient primary, urgent, and specialty care at civilian hospitals. As access to mental health care can be limited at MTFs, preserving access to mental health care for military personnel and families is an area of priority. Among TRICARE beneficiaries with access to both MTFs and civilian hospitals, 35% of admissions were at civilian hospitals.
Utilization of civilian hospitals by active-duty service members varies significantly across military installations. Some military installations, such as Vance Air Force Base in Oklahoma, lack an on-base hospital or emergency room. Vance’s 2,300 active-duty service members and their families must therefore use civilian hospitals. This may affect their continuity of care, particularly for family members with special needs for whom the military typically provides additional support.
Civilian Hospital Closures and Access to Healthcare
The dependence on civilian healthcare infrastructure raises concerns about healthcare access for active-duty service members and families when nearby hospitals face financial distress or closure. Hospital closures have accelerated in recent years, with more than 500 hospitals closing or converting to non-acute care facilities since 2010. Our prior analysis identified several reasons why hospital financial distress may accelerate in coming years, with the potential of H.R.1 (Public Law No. 119-21) to harm hospitals by limiting provider taxes and reducing Medicaid eligibility.
The following analysis estimates how many of the 8.9 million TRICARE beneficiaries in our dataset may be exposed to the hospitals that we consider to be at greater risk of financial distress. We define “potentially exposed” beneficiaries as residing in a Hospital Service Area (HSA) that contains at least one hospital in the higher-risk or moderate-risk category, regardless of where a beneficiary actually seeks care.
We begin by defining the universe of higher-risk and moderate-risk hospitals. Then, we define potentially exposed HSAs as the set of HSAs that have higher-risk and moderate-risk hospitals. Finally, we take a spatial dataset of military installations and assess the overlap between them and the potentially exposed HSAs.
Our analysis estimates that more than 117,000 TRICARE beneficiaries currently living on or near military installations are potentially exposed to a hospital at higher risk of financial distress. However, more than 3.5 million TRICARE beneficiaries are potentially exposed to a higher-risk or moderate-risk hospital. Understanding which military installations are located near financially vulnerable hospitals is critical for ensuring continuity of healthcare access for TRICARE beneficiaries.
Approach
Hospitals
We aggregated data from multiple sources to assess the exposure of TRICARE beneficiaries to hospitals at risk of financial distress. Hospitals were drawn from the American Hospital Association Annual Survey. Hospital financial data were obtained from RAND’s 2023 CMS Hospital Cost Report Data. Hospital Service Area boundaries and ZIP code crosswalks were obtained from the Dartmouth Atlas of Health Care.
TRICARE enrollment was obtained from the 2023 American Community Survey, which estimated the average enrollment by ZIP code from 2019–2023.
Based on our prior analysis, we categorized hospitals based on three risk factors for financial vulnerability:
- Structural Vulnerability, as defined by safety-net hospital status or Critical Access Hospital designation. Safety-net hospitals were defined as hospitals within the top quartile of Disproportionate Share Hospital (DSH) percentage. Critical Access Hospitals are rural hospitals that provide essential healthcare services to underserved communities.
- Financial Distress, as defined by Altman Z-score less than 1.8. The modified Altman Z-score combines measures of hospital liquidity, profitability, financial efficiency, and solvency to categorize hospitals as distressed and at high risk for bankruptcy.
- High Medicaid Payer Mix, as defined by greater than 25% patient mix from Medicaid. For this analysis, we defined hospitals in this category if they had either 25%+ of admitted patients on Medicaid (as defined by the AHA) or 25%+ of claims fulfilled by Medicaid (as defined by NASHP – the National Academy for State Health Policy).
We classified hospitals into three risk categories: Higher-Risk (all 3 risk factors present), Moderate-Risk (exactly 2 risk factors), and Lower-Risk (0 or 1 risk factors). We similarly classified Hospital Service Areas based on the highest-risk hospital present within each HSA. Hospital risk status is defined as of 2023, which is the latest year for which hospital-level financial information is available.
Military Installations
We defined military installations as sites with Air Force, Army, Marines, Navy, and/or Space Force presence and that were listed on the federal MilitaryINSTALLATIONS website. Minor installations such as weapons stations, depots, and training centers were excluded, unless the installation had housing on-site.
We identified 207 installations that met the inclusion and exclusion criteria. We defined the boundaries of each installation as the set of all ZIP codes overlapping with the U.S. Census Bureau TIGER/Line shapefile of that installation. Because several installations are close together, we combined the 207 installations into 153 “clusters.” Clusters were defined by combining installations that had ZIP codes with borders <2 miles apart. Accordingly, each ZIP code was unique to a cluster.
We then linked military installation clusters to Hospital Service Areas through their shared ZIP codes and calculated the number of TRICARE beneficiaries in each combination of military/non-military ZIP code and HSA risk category.
Findings
Hospitals and HSAs
Our sample included 4,403 general acute care hospitals and 3,436 HSAs. As shown in Table 1, most hospitals and HSAs are considered lower-risk.
Table 1: Hospitals and HSAs by Combination of Risk Factors, 2023
| Description | Total risk factors | Number of hospitals (% of all hospitals) | Number of HSAs (% of all HSAs) |
| Higher-risk | 3 | 188 (4.3%) | 161 (4.6%) |
| Moderate-risk | 2 | 856 (19.4%) | 645 (18.8%) |
| Lower-risk | 0 or 1 | 3,359 (76.3%) | 2,630 (76.5%) |
TRICARE Beneficiaries
Approximately 8.9 million TRICARE beneficiaries reside in ZIP codes that could be linked to Hospital Service Areas. Of this number, 0.98 million (11.0%) are potentially exposed to higher-risk hospitals, and 2.54 million (28.4%) are potentially exposed to moderate-risk hospitals.
Among the 8.9 million TRICARE beneficiaries, 1.71 million (19.2%) live in ZIP codes that overlap with military installation boundaries. The remaining 7.22 million (80.8%) beneficiaries live in non-military ZIP codes.
We then examined the number and proportion of beneficiaries within military installations who are potentially exposed to moderate-risk or higher-risk hospitals.
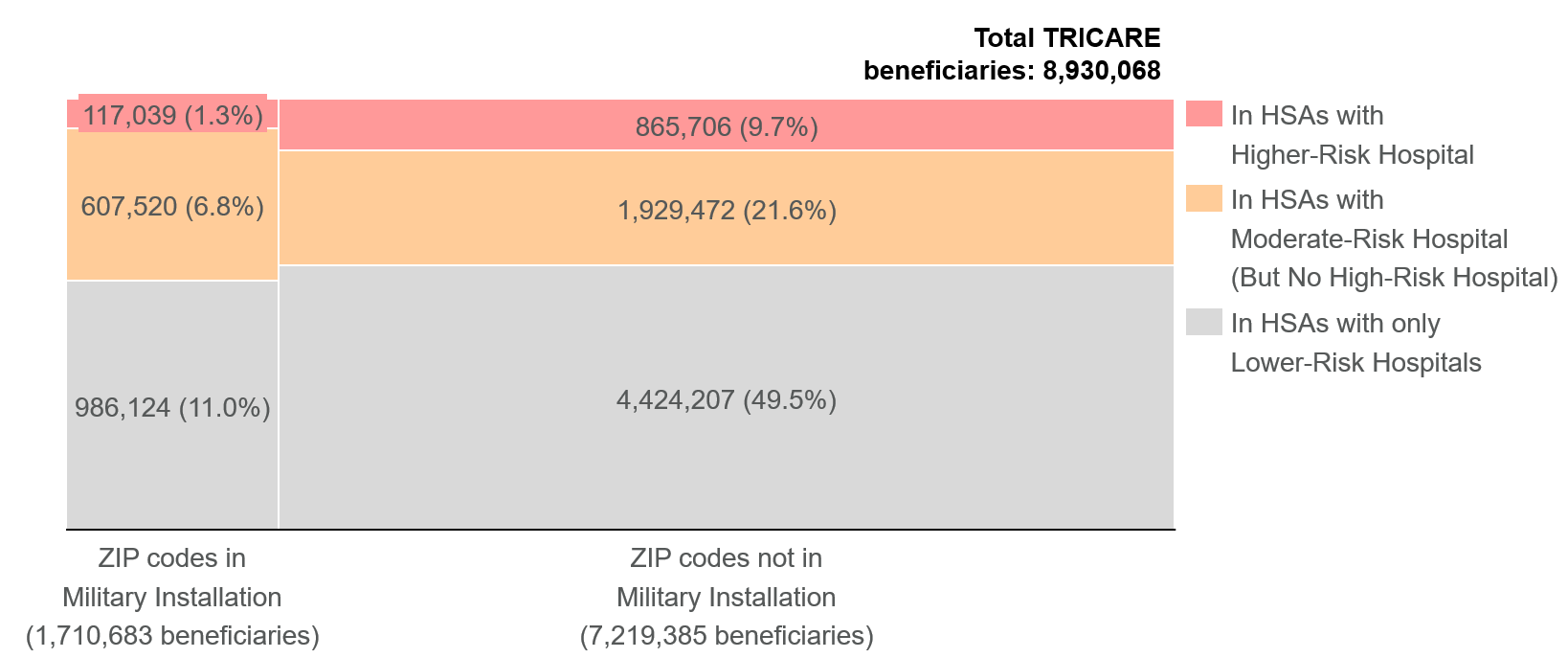
Among the 1.71 million TRICARE beneficiaries living in military installation ZIP codes, 117,039 (6.8% of all beneficiaries in installation ZIP codes) reside in HSAs containing higher-risk hospitals, and an additional 607,520 (35.5%) reside in HSAs containing moderate-risk hospitals. Combined, 724,559 TRICARE beneficiaries (42.3%) who live on or near military installations are potentially exposed to hospitals with moderate or higher risk.
Figure 1: TRICARE Beneficiaries Segmented by Exposure to At-Risk Hospitals and HSAs
Military Installation Clusters
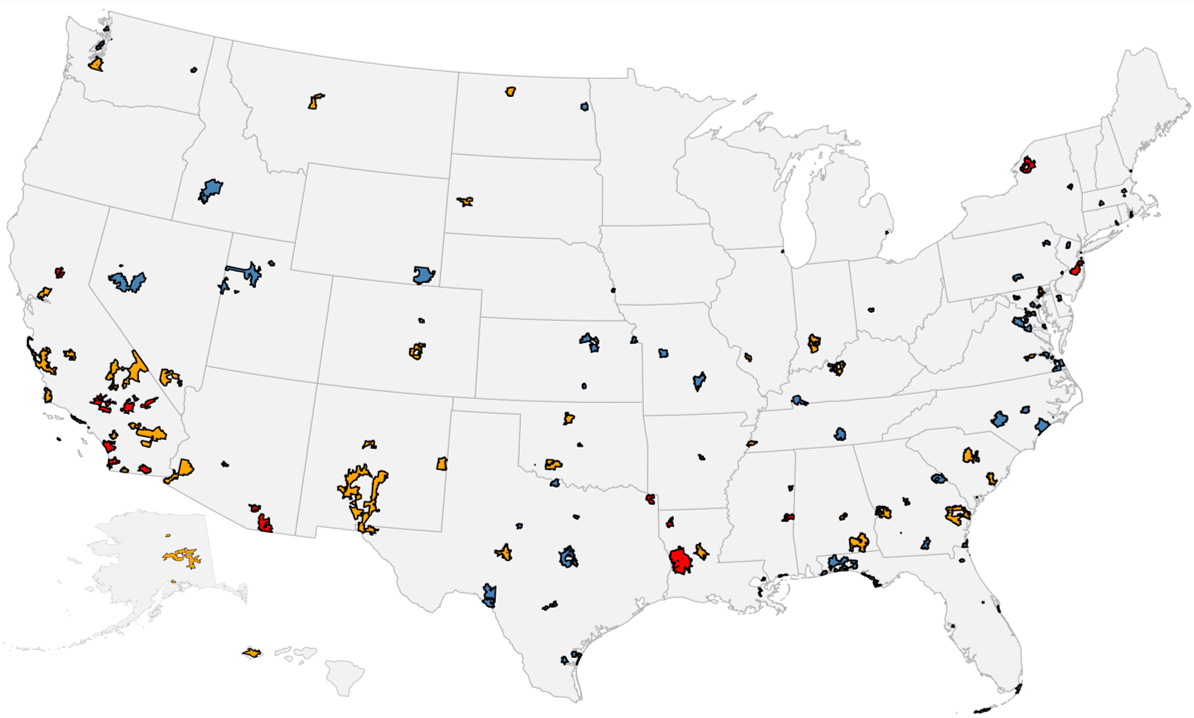
Of the 153 military installation clusters identified, 25 clusters (16.3%) are potentially exposed to higher-risk hospitals, and an additional 56 clusters (36.6%) are potentially exposed to moderate-risk hospitals but no higher-risk hospitals. Only 72 clusters (47.1%) are exclusively served by HSAs containing only lower-risk hospitals.
Figure 2: Risk Status of Military Installation Clusters by Overlap with At-Risk HSAs
Military cluster color-coding determined by highest-risk hospital in overlapping HSAs

Geographic Distribution of At-Risk Hospitals
Higher-risk and moderate-risk hospitals that serve military installations are distributed across nearly the entire country. As shown in Table 2, the 10 states with the highest number of affected TRICARE beneficiaries living on military installations come from the Southeast, Southwest, West Coast, and Midwest. No single state has more than 20% of those potentially exposed beneficiaries.
Table 2: Number of TRICARE beneficiaries living in military installation ZIP codes potentially exposed to moderate-risk or higher-risk hospitals by state, 2023
| State | TRICARE beneficiaries potentially exposed to moderate-risk or higher-risk hospitals |
| California | 125,990 |
| Texas | 99,469 |
| Washington | 65,696 |
| Colorado | 52,888 |
| South Carolina | 44,594 |
| Hawaii | 44,321 |
| Alaska | 38,894 |
| Georgia | 38,665 |
| Oklahoma | 32,812 |
| Arizona | 30,514 |
| All other states | 150,716 |
Implications
Our analysis reveals that a substantial proportion of TRICARE beneficiaries depend on hospitals that face elevated risk of financial distress. Of the 1.7 million TRICARE beneficiaries in military installation ZIP codes, more than 724,000 (42%) live in Hospital Service Areas where at least one hospital has multiple risk factors for financial distress. Additionally, nearly 2.8 million TRICARE beneficiaries living outside of military installations are potentially exposed to those higher-risk or moderate-risk hospitals. In total, more than 3.5 million TRICARE beneficiaries may be exposed, representing nearly 4 in 10 TRICARE beneficiaries.
Further analysis and resources are needed to understand the extent to which each risk factor contributes to hospital closure. Additionally, our analysis should be interpreted considering its limitations. Analyses were performed at the HSA-level; future work should evaluate TRICARE claims to assess observed utilization patterns by TRICARE beneficiaries. Additionally, the ZIP code-level of TRICARE beneficiaries and hospital financial data are from 2023, and historical data may not fully reflect the current situation.
Conclusion
Preserving access to hospital care for TRICARE beneficiaries should be a priority for both defense and health policymakers. As hospitals face mounting financial pressures, understanding which military communities are most exposed to closure risk is essential for protecting the health and readiness of the military force and their families.
For more information, contact Thomas Tsai at ttsai@hsph.harvard.edu
The Healthcare Quality and Outcomes Lab (HQO) is a state-of-the-art health services research group that produces actionable evidence to improve the quality, equity, and resilience of healthcare delivery systems.