Life after death: Helping former child soldiers become whole again

[ Fall 2011 ]
Today, among the 87 war-torn countries in which data have been gathered, 300,000–500,000 children are involved with fighting forces as child soldiers.
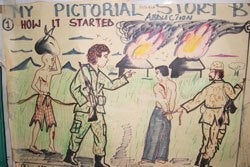
Some, as young as seven, commit unspeakable atrocities: killing parents and siblings, assaulting neighbors, torching the villages they once called home. Some are forced to serve as sex slaves. Many are injected with drugs to curb their inhibitions against committing violence.
Once the killing ends, peace treaties are signed and emergency humanitarian missions pull out. But these children’s sorrows persist.
Theresa Betancourt has made it her mission to understand how to promote their resilience—and ultimately, their healing.
From Child Soldier to Productive Citizen
Betancourt, ScD ’03, directs the Research Program on Children and Global Adversity at the François-Xavier Bagnoud Center for Health and Human Rights at Harvard School of Public Health. For nine years, she has tracked the emotional fate of former child soldiers and explored how—and if—this war-scarred cohort can go on to lead meaningful and productive lives.
Using both surveys and one-on-one interviews, Betancourt has painted a psychic portrait of young people—coolly referred to in the academic literature as “children formerly associated with armed forces and armed groups”—who struggle to find a place in tattered postwar societies. She is now adapting and testing group interventions for troubled youth in Sierra Leone that have proven successful in other places riven by violence.
Dust Cloud—or Lasting Care
“We need to devise lasting systems of care, instead of leaving behind a dust cloud that disappears when the humanitarian actors leave,” says Betancourt, who is also an assistant professor in the Department of Global Health and Population.
In Sierra Leone, assistance quickly evaporated after the African country’s crisis was no longer in the news. Today, Sierra Leone ranks 11th from the bottom on the UN Human Development Index of 169 nations. Its district health officers are justifiably preoccupied with high rates of maternal and infant mortality. The country has one psychiatrist—who practices in the capital, Freetown, and is soon to retire.
Betancourt’s research seeks to show how former child soldiers and other war-affected youth may be helped, despite such limited resources, to become contributing members of society as adults. She has disseminated her findings to hundreds of professionals from local and international NGOs and UN agencies working with Sierra Leone’s former child soldiers.

She hopes that one day these accomplishments can be bolstered by a broader continuum of care—one that extends from everyday citizens who give troubled kids encouragement and guidance to frontline community health workers to psychologists and psychiatrists, who can manage cases needing a higher level of services. In an ideal world, grassroots mental health services would offer a place for sufferers to tell their stories, talk about their dreams and ambitions, and develop trusting relationships.
“The postconflict environment is where things break down, but also where we can help,” she says. “We don’t have time to waste.”
From Alaska to Africa
Tragedy told by the numbers
|
Betancourt’s path to Sierra Leone began in the Alaskan permafrost. She was born in a Native hospital in Bethel, a town near the state’s west coast that then numbered about 3,000. Her parents, both Caucasian, imbued the family with a passion for other cultures. Her father was a math and science teacher who had joined the Peace Corps in the early 1960s, stationed in Ethiopia. Her mother worked in remote villages for the federal infant learning program.
In Bethel, where the majority of residents were Yup’ik, Betancourt acquired both an insider and outsider perspective. “My friends were Yup’ik. I had Yup’ik baby sitters. I spoke Yup’ik. We were outside the dominant culture—but we needed to understand that culture in order to live well.”
Her father’s passion for Ethiopia never waned. When friends came over for dinner, he would haul out his slide projector and display pictures from his Peace Corps days. “We were in small-town Alaska permafrost,” Betancourt says, “but we always knew what Africa looked like.”
Initially trained as a counselor using expressive arts in therapy with children, Betancourt started focusing in 1995 on children affected by war. First with the UN Office of the High Commissioner for Human Rights, then with the International Rescue Committee (IRC), a New York-based humanitarian organization, she worked with young refugees in Albania, Chechnya, and the Eritrea-Ethiopia border, organizing emergency education programs and eventually research initiatives.
In 2002, at the end of a bloody 11-year civil war, Betancourt made her initial trip to Sierra Leone to work with the boys and girls there. “The first time I met with former child soldiers, what struck me was that they looked really little, really young. They told me they were 13 and 14, but they looked eight. They were malnourished and wearing tattered clothes.
I couldn’t fathom what they had seen.”
Betancourt has now been tracking more than 500 former child soldiers, many of whom are growing into adulthood and starting their own families. Her main questions: What helps young people endure this experience and still thrive? What qualities of the individual, the family, and the environment shape resilience? How can effective interventions, resonant with the local culture, be delivered by community members who receive special training and routine supervision?
Groundbreaking Research Tells the Story
Betancourt believes both numbers and words are needed to take the measure of a child soldier’s trauma. As a result, she relies on both quantitative and qualitative methods in her research efforts. In her longitudinal study, she uses a detailed questionnaire to elicit the boys’ and girls’ war and postconflict experiences. Her local staff conduct in-depth qualitative interviews of the children and their caregivers, along with focus groups in the community.
Much of the existing scholarship on intergenerational relationships in war-exposed populations is based on the experiences of Holocaust survivors. Betancourt’s work is, therefore, groundbreaking. Her nine-year project following male and female child soldiers in Sierra Leone is Africa’s first such prospective study.
And a 2007 study that Betancourt co-authored was one of the first randomized controlled trials of mental health interventions among African adolescents affected by war—and one of only a handful of trials of psychological treatments for depression conducted in a developing country. Among other things, she has shown that effective treatments—and clinical trials of these treatments—are feasible in poor, rural, illiterate, war-torn communities.
A Vicious Circle
In Sierra Leone and elsewhere, former child soldiers suffer nightmares, intense sadness, intrusive thoughts, and recurring violent images. Not surprisingly, those who committed extreme acts of violence, or were its victims, tend to suffer the most persistent mental health problems and need the most intensive care.
Frequently, these children have difficulty with community relationships after their release. They struggle with guilt and shame. They are labeled as different or untrustworthy, which, in a vicious circle, deepens their sense of isolation. In their home communities, they are blamed for having destroyed lives, homes, property, and society itself. Those who are socially isolated are especially vulnerable to addictions and abusive relationships.
Girls face a compound burden. They are more likely to suffer depression, anxiety, and post-traumatic stress disorder, compared with boys. Some have returned to their communities having had unwanted pregnancies during their times with rebel groups. At home, they face the double stigma of having participated in violence and being seen as “impure,” regardless of their war experiences.
Hundreds Taught to Work with Former Child Soldiers
HSPH FellowshipsEn route to earning her doctorate in 2003 at HSPH, Theresa Betancourt received crucial financial aid. In 1998 and 1999, she was awarded a Taplin Fellowship, which paid her expenses. In 1998, she held a Saltonstall Fellowship at the Harvard Center for Population and Development Studies, which helped launch her field research on the Chechnya conflict. In 2008 and 2009, she received the Julie Henry Junior Faculty Development Award, which supported Betancourt’s Family Strengthening Intervention project in Rwanda, a pilot study to bolster resilience and prevent mental health problems among children in postgenocide Rwanda whose families are affected by HIV/AIDS; the research led to a National Institute of Mental Health grant.
|
To grapple with these problems, Betancourt and her colleagues have looked to existing evidence-based mental health interventions that help violence-affected youth manage their emotions and build interpersonal skills. The goal is to forge connections to families and communities, and give children the
wherewithal to negotiate the adversities they often encounter. Ideally, such approaches are linked to educational and job programs that restore civilian roles—since returning to school or securing a livelihood are prime sources of confidence and motivation in the children.
Betancourt emphasizes that direct, sustained treatment of war-affected children is the task of local partners. “I like to stay put in a place, develop relationships, and keep working at things over time,” she says. Despite the oppressive content of her work, she is neither dour nor drawn to philosophical discussions about the nature of good and evil. As she puts it, “I’m very pragmatic.” Married to a physician specializing in health inequities, and the mother of two young children, she has a noticeable lightness of spirit.
Distress Has a Local Meaning
Betancourt is planning pilot studies that use components of cognitive behavioral therapy and an approach known as group interpersonal psychotherapy that has proved successful in relieving depression among children—some former soldiers, some not—crowded in refugee camps in embattled northern Uganda. Group interpersonal therapy is based on the idea that the roots of depression, and the mechanisms for healing it, lie in people’s relationships with others. Young people who have all experienced the same ordeal can share support, wisdom, and understanding.
In Betancourt’s intervention, war-affected young people learn that they are not alone in their experiences and emotions.
“The key is being able to put a word to their feelings: sadness, worthlessness, hopelessness, loss of energy, the sense that life is not worth living,” she says. “We spend a lot of time trying to learn local terms for emotional suffering. Once intervention and problem solving begins, these young people no longer feel alone. Their symptoms start to lift.”
Betancourt and her team call their pilot model the Youth Readiness Intervention, because it builds readiness to succeed in critical aspects of life such as personal relationships, taking care of one’s self, planning for the future, and achieving economic self-sufficiency. Meeting weekly for two months, the participants focus on the present: setting goals, curbing high-risk behaviors and substance use, reducing trauma-related distress, and boosting community involvement.
Complementing African Programs and Traditions
A Recipe for resilienceFormer child soldiers are not a monolithic population of the emotionally wrecked. “When people think of child soldiers, they think of people who are terribly damaged in some way,” Theresa Betancourt says. “But I’ve seen very much the opposite: tremendous stories of resilience, of acceptance, of love in families.”
In her view, resilience springs from a complex ecology of individual traits and social forces. “In one sense, any child who made it through the war alive likely developed survival strategies to navigate a harsh and dangerous environment. Some of these young people, especially those who survived abuse, possess a sense of resourcefulness, which shows up in confidence and a sense that they can control their fate.”
Another potent factor in resilience is family connectedness. When parents openly embrace their sons and daughters and bring them back into the fold, it not only sustains the child but also sends a signal to the larger community that the boy or girl is worthy of acceptance and care. Going to school, doing homework, and graduating likewise foster a sense of normalcy and regaining lost time.
How the wider culture draws meaning from the war and its aftermath also influences the fate of former child soldiers. During the postwar, government-led process, which has included sanctioned forgiveness and community sensitization campaigns, many young people received the explicit message that their involvement in the country’s atrocities was not their fault.
|
“The groups fit well in collectivist cultures such as in Uganda or Sierra Leone,” says Betancourt. “In northern Uganda, we saw very strong effects in girls, more so than in boys. That may be because in these crowded camps—where girls had a lot of responsibilities caring for people, cooking, gathering firewood, fetching water—they didn’t have much in the way of supportive social contacts before meeting other girls in the same situation.”
Betancourt’s locally adapted models also complement what has been initiated in Sierra Leone and other nations, including “sensitization” campaigns that encourage communities to discuss the conflict and the dangers of excluding any stigmatized group. Traditional healing ceremonies—such as ritual washings and collective feasts—can also mark new beginnings for former child soldiers.
Such evidence-based interventions are far more effective than the once-popular technique in humanitarian assistance known as “psychological debriefing,” in which Western practitioners briefly visit war zones, conduct therapies in which victims talk about their traumatic experiences, then leave.
According to Betancourt, “Flying in and asking someone to share their trauma in one or two sessions, without an ongoing, safe therapeutic relationship, can actually do more harm than good.”
Not a “Lost Generation”
In the aftermath of chaotic civil wars, investments in psychosocial and mental health problems are typically phased out as the problem shifts to a postconflict and then a reconstruction phase. “Unfortunately, these children’s needs do not follow a similar phasing-out process, particularly when they have been ill-addressed at the outset,” says Betancourt. “There is real difficulty in getting funding for this work. Sierra Leone, in particular, is seen as a ‘has been’ conflict: no longer sexy.”
What most worries her is that societies will write off former child soldiers as a “lost generation.” The opposite could be true, she contends: The very qualities that helped these children survive a harrowing experience may also enable them to catalyze change in their shattered homelands.
And while Betancourt’s research may seem specialized, many of her findings transcend culture. “When someone’s a survivor, it means they are still here today, despite what they went through,” she says. “It would be terrible if people who had been through events like this saw themselves as hopeless or as victims. A survivor orientation means being able to feel the strength of what it takes to make it through such horrendous experiences and still move forward in life.”
Learn More
Register to hear Theresa Betancourt speak during our free HUBweek Panel, “Four Global Health Threats, Four Global Health Opportunities”
Madeline Drexler is editor of the Review.


